If you’ve had gout, or know anyone who’s had it, you know it’s a pain in the butt… I mean the toe! This week’s blog is about what gout is, what causes it, and what you can do about it.
Years ago, when I was a young pharmacist just beginning my career, a poor guy hobbled into the pharmacy one evening after office hours, with a loose overshoe on one foot. He had the gout, he told me, and was in terrible pain. I remembered from pharmacology classes that colchicine was a drug of choice and didn’t require a prescription at that time (that’s changed now). Our professor had stressed that colchicine quickly decreased the pain and inflammation but didn’t correct the underlying problem. So, I sold him a few tablets to get him through the night and told him to see his doctor the next day for assessment.
The next day, a gruff voice on the doctors’ line asked if I was the pharmacist who had supplied the colchicine to his patient. Nervously, I admitted yes it was me (I’d only been a pharmacist for a few months), and he said, “You did well!” Whew!! Of course, now, many pharmacists are permitted to prescribe for certain conditions, and some governments actually pay them for this service.
But what is gout anyway?
Gout is a form of inflammatory arthritis, that is caused by too much uric acid in the blood (“hyperuricemia”… hyper [too much]-uric [uric acid]-emia [in the blood]). The uric acid precipitates out of the blood, forming sharp crystals of sodium urate inside a joint, most often in the big toe because of gravity. The crystals can also form inside the ankle, knee or fingers, especially when blood uric acid is very high. In advanced long-term gout, the collection of crystals can sometimes be seen as hard bulges called “tophi” under the skin that covers the joint as the crystals expand beyond the joint.
The rough needle-like crystals scrape the inside of the joint causing pain and inflammation (redness and swelling). Anti-inflammatory drugs are generally the first treatment offered, to reduce the inflammation and control pain, and often the crystals will dissolve on their own.
Where does uric acid come from?
Uric acid is created in the body when we break down purines, a component of DNA in human and animal cells known as nucleosides, essential for life. So, animal and human cells all contain purines that are used when the cells grow and divide. Plants contain them too, but generally in lower amounts.
We get purines in our diet when we eat anything that was living, but plants are not considered a significant source. It is animal protein, especially red meat, organ meats, some types of alcohol (beer), some seafood (sardines, anchovies), and high fructose foods (soft drinks) that contain the highest amounts of purines. Foods low in purines include eggs, nuts, legumes, fruit, whole grains, vegetables (except asparagus, cauliflower, spinach, mushrooms, and green peas have relatively more), dairy products, poultry, crab, salmon and herring.
I’m sure I remember learning that alcohol makes uric acid less soluble (and therefore, more likely to form urate crystals) but I’m not seeing that in the literature now…
Quick chemistry lesson… Skip this section if you hate chemistry!! ��
DNA is the genetic material in the nucleus of every cell that carries the programming information to make proteins that do the work in our bodies. Purines and their partners, the pyrimidines form the “bridges” between the 2 backbones of the DNA double-helix, creating the twisted ladder of DNA that’s familiar to most of us.

There are 2 purines (adenine and guanine) and 2 pyrimidines (thymine and cytosine), and they always pair up, one of each, the same way. This ensures that when a cell divides and the strands of DNA split apart, they always match up correctly, creating 2 new cells with the same DNA as the original. Each group of 3 “bridges” codes for one amino acid, and a series of amino acids creates a protein that could become an enzyme used to build a structure in the body or enable a chemical reaction that has a function.
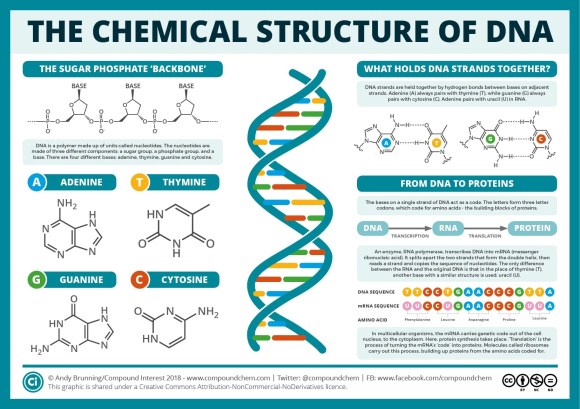
A picture is worth a thousand words, isn’t it?
Basically, we make our own purines as well as get them in our food. Any increase in protein breakdown (which would increase purines that need to be eliminated) or reduction in elimination of purines can result in increased blood uric acid. A defect in the genes that create enzymes that manufacture or breakdown purines can also result in an increased risk of gout, so sometimes gout runs in families.
Uric acid is cleared from the body by the kidneys in the form of urea in the urine so if kidney function is poor, uric acid clearance is reduced. Many kidney stones are made of urate crystals (equally sharp!) and the process is probably similar. Not surprisingly, there’s a tie between kidney stones and gout—kidney disease can cause gout (because of reduced clearance of uric acid/urea) and gout can cause kidney disease (lots of uric acid available to form those nasty kidney stones that scrape the inside of the kidney).
And when more cells than usual are broken down, for example during cancer therapy, more purines are freed-up to be metabolized and can overwhelm the body’s ability to keep up, resulting in increased blood uric acid. I remember my Dad having gout during his leukemia treatments, years ago.
OK, enough biochemistry… here’s how it’s treated
If a person only has occasional attacks of gout, anti-inflammatories or corticosteroids (also anti-inflammatory) are used to relieve pain and swelling, until the body clears the urate crystals from the joint, usually within a few days to a few weeks, depending on how severe the attack. Later repeated attacks tend to last longer. The pain is usually most severe in the first 4 to 12 hours, with lingering soreness as the joint heals.
If the gout is continuous or reoccurs frequently, it makes sense to correct the cause rather than continue to just treat the symptoms. This is done by changing the diet and/or taking a medication to reduce the amount of uric acid in the blood.
So, in addition to choosing foods that are lower in purines to prevent gout, we also have medicines that can slow down purine metabolism, by partially blocking one of the enzymes that break down adenine and guanine, allowing the body to keep up to the production of uric acid. There are two: allopurinol (Zyloprim and generics) and febuxostat (Uloric). An anti-inflammatory may be continued for the first few weeks of this therapy, until blood uric acid is normalized, to prevent return of symptoms.
You’ll remember the drug colchicine, a strong anti-inflammatory I talked about at the beginning of this article, and other anti-inflammatories are used too, such as indomethacin, celecoxib, and the non-prescription drugs, naproxen and ibuprofen, in less severe attacks. Corticosteroids are sometimes prescribed, and colchicine is now considered 2nd line in some jurisdictions due to side effects (digestive problems, possibility of bone marrow suppression) especially if used long-term.
And another prescription drug, probenecid, is sometimes used to increase the kidneys’ ability to remove uric acid from the body.
What can you do?
- Choose healthier drinks… limit alcoholic beverages, avoid drinks sweetened with fructose. Instead drink plenty of water.
- Avoid foods high in purines… red meat, organ meats (like liver), high-purine seafood (anchovies, sardines, mussels, scallops, trout, and tuna). Low-fat dairy products may be a better source of protein for those prone to gout.
- Exercise regularly and maintain a healthy weight… excess weight can increase risk of gout. Choose low-impact exercise like walking, biking and swimming, as these are easier on the joints.
But be sure to see your doctor for a correct diagnosis, and to help you decide what level of treatment you need. Gout is sometimes confused with a joint infection, or other types of arthritis (such as rheumatoid/inflammatory arthritis). When severe enough and left untreated for too long, gout can develop into gouty arthritis with resulting permanent damage to joints.
If you found this article helpful, please like or comment so others will be more likely to see it. And, if you know someone who might benefit from this information, consider forwarding this to them!
References:
The chemical structure of DNA (diagram and explanation)
Hyperuricemia—Wikipedia
Purine—Wikipedia
Foods High in Purines—WebMD
Gout—Centers for Disease Control and Prevention (CDC)
Gout—Mayo Clinic
Photo credits:
https://www.cefootandankle.com/blog/gout/
#gout #UricAcid